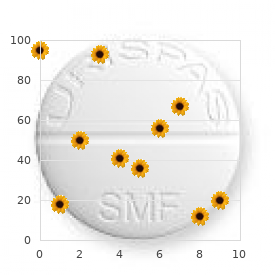
It is pointless to say that weak erectile dysfunction treatment generic 20 mg tadalis sx with mastercard, presently female erectile dysfunction drugs order 20mg tadalis sx amex, many national health-care methods provide therapies to patients with main lymphedema in an equitable method, with poor distribution of health-care sources. In most countries, the prices of supplies, elastic clothes, and medicines are charged to the patient. But, a concrete indication for the intervention among the candidates nonetheless have to be higher outlined to guarantee scientific success. Acute remedy often requires close monitoring for twenty-four hours, particularly in patients over the age of sixty five years, for potential problems similar to heart failure or temporary and reversible renal insufficiency, which may be brought on by the obstruction of the renal tubules as a end result of the high concentrations of proteins removed from the tissues in a brief while. For instance, in advanced medical phases, fast reabsorption of the protein part of edema might end in cardiac overload by increased preload and ought to be anticipated. And it might be necessary to modify the decongestive therapy, splitting it over time, and finally, associating it with a brief period of diuretic therapy to avoid possible issues and to permit higher compliance of the patient. The diagnosis and remedy of peripheral lymphedema: 2013 Consensus Document of the International Society of Lymphology. This old idea has now turn into out of date, as a result of our much-improved understanding of the nature of persistent lymphedema. Chronic lymphedema is now thought-about a "dynamic" condition with fixed interaction between the lymphatic system and the encircling delicate tissue. This is, therefore, a serious condition involving the tissues beyond the lymphatics and lymph nodes, typically related to many doubtlessly severe issues: local/ regional/systemic sepsis brought on by bacterial and fungal an infection, dermato-lipo-fibrosis, immunodeficiency-related various phenomena, and malignancy. Noninvasive analysis of the swollen extremity: Experiences with 190 lymphoscintigraphy examinations. For instance, among the many patients in the same clinical stage, the one with the extra superior laboratory stage has proven an inclination to progress sooner so that this newly added laboratory stage has been used as one of the criteria to determine which lymphedema patients would profit to proceed to incorporate additional therapy modalities with no delay, significantly surgical remedy before additional disease deterioration. Indeed, this combined approach is ready to present crucial data on the decision-making course of for supplemental surgical therapy to select the suitable timing of surgical intervention earlier than irreversible development of illness occurs. Popliteal node visualization throughout commonplace pedal lymphoscintigraphy for a swollen limb indicates impaired lymph drainage. Current standing of lymphatic reconstructive surgery for persistent lymphedema: It is still an uphill battle! Current issue in management of continual lymphedema: Personal reflection on an expertise with 1065 patients. Section Diagnosis 13 forty eight Ultrasonographic assessment of lymphatic malformations-Lymphangioma and primary lymphedema: A new role for prognosis Erica Menegatti and Sergio Gianesini 49 Radionuclide lymphoscintigraphy-Gold standard for evaluation of lymphatic malformation: Lymphangioma and first lymphedema or both Vaughan Keeley 50 Magnetic resonance imaging and magnetic resonance lymphangiography of primary lymphedema: A new gold commonplace Ningfei Liu fifty one Indocyanine green fluorescent lymphography: Clinical implementation Takumi Yamamoto fifty two Oil distinction lymphangiography: New position for the surgical candidate Francesco Boccardo, Sara Dessalvi, Corrado Cesare Campisi, and Corradino Campisi fifty three Fluorescent microlymphangiography: Controversy, confusion, and neglected problems Claudio Allegra, Michelangelo Bartolo, and Salvino Bilancini fifty four Can indocyanine green exchange function of lymphoscintigraphy Takumi Yamamoto fifty five How to differentiate between lymphedema and lipedema: How to rule out lipedema " " Gyozo Szolnoky 217 221 225 229 233 239 243 245 48 Ultrasonographic assessment of lymphatic malformations-Lymphangioma and first lymphedema: A new role for analysis Most of these lesions are already current at birth or appear within 2 years of life. Chronic lymphedema is characterized by pores and skin thickening and tissue fibrosis; it presents indicators of irritation and nonpitting pores and skin texture. The former presents as multilocular cystic plenty with massive thin-walled cysts containing variable echogenicity. Vascular anomalies classification: Recommendations from the worldwide Society for the Study of Vascular Anomalies. High-resolution cutaneous ultrasonography to differentiate lipedema from lymphedema. Subsequently, a sequence of images are obtained utilizing a -camera, and from these, features such as the velocity of motion of tracer from the injection site to the regional lymph nodes, the presence of abnormal collateral flow pathways. Quantitative imaging demonstrates very reduced uptake by the ilioinguinal lymph nodes. In lymphedema distichiasis, the injected tracer travels quickly up to the regional lymph nodes however refluxes to the pores and skin giving the looks of dermal backflow as a result of the lymphatic valvular incompetence typical of this condition. A latest research emphasised the importance of this method and that delayed circulate may be the solely abnormality seen in some instances of lymphedema. Lymphoscintigraphy reveals a traditional sample in unaffected right leg however delayed move and dermal backflow within the left foot. In those with suspected primary lymphedema, the sensitivity was 97% and the specificity 78%. Popliteal nodes within the left leg demonstrating rerouting by way of the deep subfascial lymphatics. It might, however, have a task in the further phenotyping of lymphatic abnormalities in major lymphedema. These could be affected in some advanced types of main lymphedema and in some lymphatic malformations. Importance of accurate ilio-inguinal quantification in lower extremity lymphoscintigraphy. The classification and diagnostic algorithm for main lymphatic dysplasia: An update from 2010 to embody molecular findings. Diagnostic accuracy of lymphoscintigraphy for lymphedema and analysis of false-negative tests. Magnetic resonance imaging versus lymphoscintigraphy for the evaluation of focal lymphatic transport issues of the lower limb: First experiences. Comparison of lymphoscintigraphy and indocyanine green lymphography for the prognosis of extremity lymphoedema. Modern strategies of lymphangiography and interventions: Current standing and future improvement. The comparatively uncommon forms of primary lymphedema are: unilateral lymphedema of an upper extremity, facial, and isolated exterior genital lymphedema. In common, external genital lymphedema is related to edema of the lower limb(s). In very uncommon cases, lymphedema happens in multiple sites, such as the ipsilateral face, higher and lower limbs, or contralateral higher and decrease extremities. The lymphatic system is composed of pre-collecting, amassing lymph vessels (afferent and efferent) and lymph nodes. The pre-collecting vessel is between the capillary vessels and accumulating vessels. The lymphatic malformations in major lymphedema can happen at any stage of the lymphatic system. Currently, lymphedema, especially primary lymphedema, remains an "incurable" condition till a causal genetic defect is correctly corrected or compensated. The lack of efficient therapy is due largely to lack of exact diagnostic modality to understand the pathological adjustments of the lymphatic system. Under heavy T2-weighted imaging, the static or motionless fluid (lymph within the vessels and edema fluid within the tissues) shows high signals. When the background is saturated, lymph flow itself might act as a contrast medium to spotlight the trail of the lymphatic channels. The enlarged lymphatic vessels with channels (approximately 1 mm or more) and native dilated lesions could be clearly depicted. The enhancement of those lymphatic pathways continued all through the examination time, around forty minutes. On the initial pictures, the enhancement of lymphatic channels may be light and discontinued. But the sign depth elevated, and the channels progressively turned completely opacified with time. Clusters of dilated inguinal, iliac, scrotum, and lumbar trunks (arrowhead) are additionally visualized. The variety of contrast-enhanced lymphatics in lymphedematous limbs various from single to quite a few. The form of inguinal lymph node within the contralateral facet of healthy volunteers are spherical or oval, numbered from 2�3 to 7�8 with a diameter around 1 cm.
Hereditary liver ailments that produce hepatocellular harm are Wilson illness erectile dysfunction caused by high blood pressure medication purchase tadalis sx 20 mg, hemochromatosis impotence cure discount 20 mg tadalis sx with visa, and 1antitrypsin deficiency. Congestive and ischemic disease within the liver is caused by congestive coronary heart failure, constrictive pericarditis, hypotension, portal vein thrombosis or hepatic vein outflow obstruction from Budd�Chiari syndrome, inferior vena cava occlusion, or venoocclusive illness. Significant liver illness during being pregnant, similar to acute fatty liver of being pregnant and hepatocellular damage secondary to toxemia, usually happens within the third trimester. Medication induced and toxininduced causes of harm are very common and require a excessive index of suspicion and careful questioning. Clinical presentation History An correct historical past is crucial for a patient whose laboratory research present proof of liver illness. Many conditions that produce abnormal liver chemistry ranges are painless, but acute biliary obstruction from stones can produce intense proper upper quadrant ache. Acute hepatitis produces less welldefined right upper quadrant discomfort with profound fatigue, whereas hepatic tumors may cause subcostal aching. The Patient with Jaundice or Abnormal Liver Biochemical Tests 135 Exposure to ethanol and industrial and environmental toxins must be recognized. A detailed treatment historical past, including overthecounter and natural cures, is crucial. In particular, the usage of episodic or intermittent medicines, such as steroid tapers for asthma or antibiotics, might require specific questioning. Alcoholic patients should be questioned about acetaminophen use because hepatotoxicity can happen in these individuals with therapeutic dosing because of cytochrome P450 induction. Intravenous drug abuse, sexual contact, and blood transfusions are related to a danger for viral hepatitis B or C, whereas sudden worsening of liver chemistry levels in a continual hepatitis B provider suggests attainable hepatitis D superinfection. Waterborne outbreaks of viral hepatitis have been reported in South East Asia and India, underscoring the significance of acquiring a travel historical past. Risk elements for hepatitis A include current ingestion of raw or undercooked oysters or clams, male homosexuality, or exposure through day care. Right sided congestive coronary heart failure, hypotension, and shock are recognized causes of irregular liver chemistry findings. Chronic pancreatitis may produce abnormal liver checks because of stenosis of the frequent bile duct. Obesity, hyperlipidemia, diabetes, and corticosteroid use are risk elements for nonalcoholic fatty liver illness. Rashes, arthritis, renal disease, and vasculitis could develop with viral hepatitis. The presence of hypogonadism, coronary heart illness, and diabetes suggests possible hemochromatosis. Concurrent lung disease could occur with 1antitrypsin deficiency, and central nervous system findings are related to Wilson disease. Renal cell carcinoma manifests as abnormal liver chemistry ranges within the absence of metastases. Recent surgery must be famous because anesthetic exposure, perioperative hypotension, and blood transfusions all may have an result on the liver. Cirrhosis is a late complication of jejunoileal, but not gastric, bypass surgery for morbid weight problems. Physical examination Physical findings are of discriminative value for a affected person with abnormal liver chemistry findings. Spider angiomas, palmar erythema, parotid enlargement, gynecomastia, a Dupuytren contracture, and testicular atrophy are stigmata of continual liver illness, usually cirrhosis, although many of those indicators have low specificity. A liver span greater than 15 cm suggests passive congestion or liver infiltration. A pulsatile liver suggests tricuspid insufficiency, and hepatic bruits or rubs raise the potential of hepatocellular carcinoma. Occult or gross fecal blood on rectal examination suggests attainable inflammatory bowel disease or neoplasm. A subset of patients in whom the checks for the above viral markers have adverse outcomes will exhibit constructive serological findings for cytomegalovirus, herpes simplex, coxsackievirus, or Epstein�Barr virus. Copper storage variables Ceruloplasmin is a copper transport protein in the plasma that circulates in low concentrations in Wilson disease; low levels (<20 mg/dl) are measured in 90% of homozygotes and 10% of heterozygotes. Reduced ranges may happen with severely depressed synthetic function brought on by other endstage liver ailments. Alternative diagnostic checks for Wilson illness embody urinary copper, which exceeds 100 mg per 24 hours in practically all patients, and free serum copper, which is markedly elevated. Iron storage variables Serum iron level and total ironbinding capacity (transferrin) are useful measures in diagnosing hemochromatosis. A transferrin saturation larger than 45% will determine more than 98% of patients with hemochromatosis. Elevations in serum iron with normal transferrin saturation occur in alcoholic liver disease. A liver biopsy may be required for older patients with high ferritin ranges to quantify tissue iron and to determine the extent of fibrosis, which is able to information the need for screening for hepatocellular carcinoma. Phenotyping is more accurate for prognosis than dedication of serum ranges of the protein. Percutaneous liver biopsy As a basic rule, direct forms of liver harm are most likely to cause predominant centrizonal necrosis; immunologically mediated forms of hepatocyte damage are localized to the periportal region; and cholestatic damage is recognized by the accumulation of canalicular bile and feathery degeneration of hepatocytes in the absence of a big inflammatory infiltrate. Clinical functions of liver biopsy embrace evaluating persistently irregular liver chemistry levels, establishing the prognosis in unexplained hepatomegaly, and evaluating suspected systemic disease or carcinoma involving the liver. Contraindications to liver biopsy are an uncooperative or unstable patient, ascites, rightsided empyema, and suspected hemangioma. For patients with ascites or an increased risk of bleeding, a transjugular method is an alternative selection to the percutaneous method. Management Liver disease is classified into three groups: cholestatic, hepatocellular, and infiltrative. Cholestatic liver illness often ends in increased serum bilirubin and alkaline phosphatase levels with regular to mildly elevated aminotransferase ranges, although transient profound aminotransferase elevations might happen in early biliary obstruction. In partial biliary obstruction, the bilirubin stage may stay normal in the face of an elevated alkaline phosphatase concentration. The most direct approach to evaluating suspected cholestasis is performing ultrasound to assess bile duct size. In questionable circumstances, percutaneous liver biopsy could present a definitive diagnosis. Prolongation of prothrombin time and decreases in serum albumin ranges indicate significant hepatic synthetic dysfunction. In patients with acute malaise, anorexia, nausea, jaundice, tender hepatomegaly, and elevated ranges of aminotransferases, serum ought to be screened for viral markers to exclude hepatitis A, B, or C infection, relying on the patient danger elements. With disease duration of greater than six months, additional the Patient with Jaundice or Abnormal Liver Biochemical Tests 141 research. A hepatocellular sample is noticed with ischemic and congestive liver illness, but measures to enhance hepatic blood flow in these situations can produce brisk reductions in aminotransferases to near normal ranges inside 48�72 hours. With congestive liver disease, the prothrombin time may be extended out of proportion to other signs of liver illness. If aminotransferase levels remain high for longer than six months without an identifiable cause, a liver biopsy is indicated for prognosis and to supply prognostic details about possible progression to cirrhosis. Many persons with persistently high aminotransferase ranges are obese or use ethanol, and the standard finding on liver biopsy is fatty liver illness within the absence of serological prognosis. However, the sudden discovering of persistent energetic hepatitis in a subset of these sufferers supplies support for biopsy even in asymptomatic people. Key follow factors � Liver chemistries present data regarding liver function and serve as markers of hepatobiliary illness. Case studies Case 1 A 67yearold girl is referred to the hepatology clinic with issues for potential cirrhosis. Her physical examination notes the absence of hepatosplenomegaly, however she has pitting edema of her decrease extremities. On evaluate of her medical historical past, you note she has longstanding diabetes difficult by extreme gastroparesis. You further suspect that she is malnourished as a outcome of her gastroparesis, and you present her with vitamin K supplementation. Followup laboratory values after several months reveal improved serum albumin to three. Protein losses because of proteinuria, proteinlosing enteropathy, and malnutrition may find yourself in marked hypoalbuminemia. The use of antibiotics and anticoagulants can extend the prothrombin time, as can persistent cholestasis, steatorrhea, and malnutrition.
Change of garments is repeated by the patient after one other 2 days before a hospital discharge erectile dysfunction reddit order 20 mg tadalis sx with amex. The commonplace glove and gauntlet are often modified to the made-to-measure glove on the end of the stay smoking erectile dysfunction statistics order generic tadalis sx on-line. The patient alternates between the 2 sets of clothes (two sleeves and two gloves) in the course of the first week at residence, changing them every different day so that a clear set is at all times put on after showering and lubricating the arm. Note the tourniquet, which has been removed at the right, and the concomitant reactive hyperemia. After initiating compression therapy, the custom-made garment could additionally be taken in at each visit using a stitching machine, to compensate for lowered elasticity and lowered arm quantity. The aspirate sediments into an higher adipose fraction (90%) and a lower fluid (lymph) fraction (10%). Note the sharp border between handled (distal forearm) and untreated (proximal arm) areas. How liposuction helps 301 alternative is to order a leg-length garment without the foot a part of one of the garments. The displaced water is weighed on a balance to the closest 5 g, comparable to 5 mL. Both extremities are all the time measured at each visit, and the difference in volumes is designated because the edema quantity, or extra appropriately the excess volume. The decrease within the extra volume is calculated in a share of the preoperative value. If that is the case, it is essential to keep in mind to prescribe clothes for six months. When the excess quantity has decreased as a lot as attainable and a steady state is achieved, new garments can be prescribed using the latest measurements. In this manner, the garments (two units of sleeve and glove garments) are renewed three or four occasions through the first year. The affected person is knowledgeable about the significance of hygiene (daily shower with soap and water) and skin care (moisturizing the skin with lotion), as all sufferers with lymphedema are vulnerable to infections. After complete discount has been achieved, the affected person is seen every year when new garments are prescribed for the approaching yr, normally four clothes and 4 gloves (or 4 gauntlets). In energetic sufferers, six to eight garments and the identical quantity of gauntlets/gloves a 12 months are wanted. The bigger the diameter of the leg, the more compression is needed based on the legislation of Laplace. A typical example is Elvarex compression class three, Elvarex compression class 2, and Jobst Bellavar compression class 2. It is essential to take unfastened measurements at the ankle for the explanation that diameter right here is small, giving extra compression than needed. An To investigate and treat sufferers with lymphedema, a group comprising a plastic surgeon, an occupational therapist, and a physiotherapist is needed. An hour is reserved for each scheduled go to to the team when arm volumes are measured, clothes are adjusted or renewed, the social circumstances are assessed, and other issues of concern are mentioned. The patient can be inspired to contact the team every time any surprising problems arise, in order that these may be tackled at once. The group additionally screens the long-term consequence, and a go to every year is important, generally, to preserve an excellent functional and beauty outcome after complete discount. This routine omits any repeated "maintenance treatment," since if the excess quantity will increase, it depends on much less patient compliance or worn out garments. Also, one visit a yr is economical as in comparison with conservative treatment, where sufferers are prescribed massage as quickly as per week and repeated maintenance therapies lasting 1�2 weeks. Scintigraphies were carried out earlier than liposuction, with and with out sporting a garment. In conclusion, it was found that the already decreased lymph transport was not additional decreased after liposuction. If not, or improperly treated, the swelling will increase in time and might find yourself in a fair bigger pitting edema with concomitant adipose tissue formation. To standardize the pitting check, an examiner should press as exhausting as tolerable by a affected person with the thumb on the region to be investigated for 1 minute for arms and as much as 3 minutes in legs. When a patient has been treated conservatively and reveals no or minimal pitting, liposuction could be performed. The cancer itself is a fear, however the swollen and heavy arm introduces a further handicap for the patient from a physical, psychosocial, and psychological point of view. Physical issues include pain, limited limb motion and physical mobility, and problems with clothing, thus interfering with everyday actions. Also, the heavy and swollen arm is impractical and cosmetically unappealing, all of which contribute to emotional misery. The term edema is improper at this stage because the swelling is dominated by hypertrophied adipose tissue and never by lymph. Patients with more pitting should be handled conservatively till the pitting has been decreased. The cause for not doing liposuction in a pitting edema is that liposuction is a technique to take away fats, not fluid, even when theoretically it could take away all the accumulated fluid in a pitting lymphedema with out excess adipose tissue formation. Another reason is that a patient with out pitting is a compliant patient, who can tolerate steady compression. Any affected person with a nonpitting swelling that causes a considerable decreased high quality of life is normally a candidate for surgery. As in conservative treatment, the lifelong use (24 hours a day) of compression garments is mandatory for maintaining the impact of surgical procedure. Liposuction normalizes lymphedema induced adipose tissue hypertrophy in elephantiasis of the leg-A prospective examine with a ten-year follow-up. Liposuction provides full discount of arm lymphedema following breast most cancers treatment-A 5-year prospective study in a hundred and five patients with out recurrence. Factors that influence the incidence of brachial oedema after remedy of breast most cancers. Incidence and time path of lymphedema in sentinel node unfavorable breast cancer sufferers: A systematic evaluation. Tissue tonometry earlier than and after liposuction of arm lymphedema following breast cancer. Quality of life following liposuction and conservative treatment of arm lymphedema. Liposuction combined with managed compression therapy reduces arm lymphedema more effectively than managed compression therapy alone. Assessment of subfascial muscle/water and fats accumulation in lymphedema patients using magnetic resonance imaging. The management of lipolysis in perinodal and different adipocytes by lymph node and adipose tissue-derived dendritic cells in rats. Changes in adipocytes and dendritic cells in lymph node containing adipose depots throughout and after many weeks of gentle inflammation. Lymphatic vascular defects promoted by Prox1 haploinsufficiency cause adult-onset obesity. Outcomes of vascularized lymph node switch and lymphovenous anastomosis for remedy of main lymphedema. Use of a tourniquet with and with out adrenaline reduces blood loss during liposuction for lymphoedema of the arm. Manual lymphatic drainage adds no further quantity discount to complete decongestive remedy on breast cancer-related lymphoedema: A multicentre, randomised, single-blind trial. Liposuction of postmastectomy arm lymphedema decreases the incidence of erysipelas. Liposuction of postmastectomy arm lymphedema utterly removes extra quantity: A 13 yr research (Quad erat demonstrandum). Additionally, sufferers with lipedema endure from ache with strain or spontaneous ache of the soft tissue in affected areas. The actual term lipedema is a misnomer term, because it evokes the idea of swelling as a outcome of fluid accumulation.
For sufferers with persistent nausea weight lifting causes erectile dysfunction order tadalis sx discount, vomiting erectile dysfunction treatment needles order tadalis sx cheap, and ache nasoenteric feeding is really helpful. Total parenteral nutrition ought to be considered for sufferers with pronounced ileus who fail enteral diet trials. Resolution of pain and emergence of starvation reliably indicate that the patient is able to eat in patients with mild acute pancreatitis. The threat of recurrent gallstone pancreatitis is up to 33%; subsequently, all patients ought to endure expeditious and definitive surgical therapy. Chronic Pancreatitis Clinical presentation Chronic pancreatitis implies irreversible morphological and practical injury to the pancreas. The scientific distinction between acute recurrent pancreatitis with restoration of regular pancreatic function and construction between attacks, and persistent pancreatitis may be troublesome. Ethanol use accounts for many cases of chronic pancreatitis within the United States whereas in Asia and Africa, malnutrition is the major cause (Table 31. Most circumstances are in all probability subclinical; solely 5�10% of heavy ethanol customers develop medical pancreatitis. Abdominal pain and malabsorption are the commonest scientific options of persistent pancreatitis. Pain, which is current in 85% of sufferers, is prone to be brought on by noxious stimulation of peripancreatic afferent nerves or increased intraductal strain. Morphological studies show that the pancreatic nerves are bigger and more quite a few in sufferers with chronic pancreatitis. Patients may report regular, unremitting pain or a quantity of days of pain with painfree intervals. Food ingestion will increase the intensity of ache, leading to a worry of consuming (sitophobia), which is the primary reason for weight loss in early chronic pancreatitis. Maldigestion is the physiological defect that occurs when the exocrine operate is less than 10% of normal. Steatorrhea is the preliminary manifestation of malabsorption; azotorrhea happens in additional advanced disease. Because the mucosal absorptive capacity is intact, voluminous diarrhea is unusual; most sufferers complain of cumbersome or greasy stools. A sample of steatorrhea and weight loss within the absence of belly ache is widespread in idiopathic continual pancreatitis. Patients with ethanolinduced persistent pancreatitis might have symptoms of liver disease, including ascites, encephalopathy, variceal bleeding, and jaundice. Jaundice can even result from compression or stricturing of the intrapancreatic portion of the common bile duct. Physical examination findings may be regular or there may be marked belly tenderness. Patients might have stigmata of continual alcoholism together with gonadal atrophy, gynecomastia, and palmar erythema. Diagnostic investigation Laboratory studies the findings of laboratory evaluation are often normal in chronic pancreatitis. Patients not often exhibit hyperbilirubinemia and abnormal liver chemistry levels because of concurrent alcoholic liver illness or common bile duct stricture. Because azotorrhea happens only in superior illness, serum albumin ranges often are regular despite profound weight reduction. Serum amylase and lipase levels may be slightly elevated but marked elevations, as noticed in acute pancreatitis, are uncommon. If exocrine perform is severely impaired, serum lipase ranges could additionally be low, whereas Pancreatitis 343 serum amylase ranges normally are regular on this setting as a end result of salivary amylase manufacturing is normal. Assessment of pancreatic exocrine function Numerous methods for assessing pancreatic enzyme output can be found. The easiest exams are those who detect elevated fat in the stool, which develops if exocrine secretion is less than 10% of regular. Steatorrhea could also be detected by qualitative fecal fats exams (Sudan stain) or quantitative 72hour fecal fats measurements. In severe circumstances, the amount of fats excreted within the feces could method the quantity of fats ingested, which is indicative of profound reductions in pancreatic enzyme output. Such high levels of steatorrhea are rarely observed with mucosal illness of the small gut. Chronic pancreatitis is characterized by decreased secretory output in response to these stimulants. Incomplete duodenal recovery of pancreatic juice or gastric acid inactivation of enzymes may result in underestimation of pancreatic operate. The sensitivity of pancreatic operate checks for detecting persistent pancreatitis is 70�95%, which includes most patients with solely mildtomoderate pancreatic insufficiency. The findings from a Schilling check are abnormal in persistent pancreatitis due to impaired cleavage of R protein, which prevents the binding of vitamin B12 to intrinsic issue. Expanding this test to embrace vitamin B12 bound to intrinsic factor can differentiate the maldigestion of R protein from the malabsorption of the vitamin B12�intrinsic issue complex. Structural studies Confirming the analysis of chronic pancreatitis usually requires imaging studies of the pancreas. Abdominal radiography demonstrates the diagnostic finding of pancreatic calcifications in 30�40% of sufferers with persistent pancreatitis. Ultrasound has a sensitivity of 70% and a specificity of 90% for detecting persistent pancreatitis. Management and course Medical therapy Medical remedy for chronic pancreatitis focuses on relief of pain and repletion of digestive enzymes. If the affected person has symptoms of maldigestion, pancreatic enzyme dietary supplements must be taken earlier than all meals. At least 25,000�30,000 items of lipase per meal are necessary to present enough lipolysis; therefore, sufferers will want to take 2�10 drugs with each meal, depending on the preparation. Analgesics stay the first means of controlling the ache of chronic pancreatitis. Severe cases require opiate analgesics and comanagement with a chronic ache administration specialist. The somatostatin analog octreotide inhibits pancreatic secretion and has visceral analgesic effects; thus, it might be expected to decrease ache in persistent pancreatitis. Octreotide may also have a role in managing refractory pancreatic fistulae or pseudocysts. Nonmedical therapy A small percentage of sufferers are refractory to medical measures and require extra invasive procedures to control pain. Although celiac plexus neurolysis has been efficient for ache management in patients with pancreatic adenocarcinoma, leads to patients with continual pancreatitis have been disappointing. Endoscopic pancreatic stone extraction, occasionally carried out in conjunction with extracorporeal shock wave lithotripsy, reduces pain in 50�80% of instances. Patients with tight strictures might obtain pain aid after endoscopic balloon dilation and stent placement. For severe debilitating ache unresponsive to medical therapy, surgical therapy is a respectable technique of restoring the quality of life to a affected person with persistent pancreatitis. Patients with dilation of the main pancreatic duct are optimal candidates for pancreaticojejunostomy (modified Puestow procedure), a procedure with initial success charges of 80%. Unfortunately, many patients develop recurrent pain several years postoperatively. Patients without significant ductal dilation could Pancreatitis 345 require partial or subtotal pancreatectomy based on the extent of parenchymal disease. Pancreatic islet cell autotransplantation on the time of the operation could prevent postoperative diabetes. Complications Patients with chronic pancreatitis who report extreme refractory ache or worsening of pain should be evaluated for the development of a pseudocyst. They might rupture, bleed, or turn into infected; the risk of these issues is far decrease than the corresponding threat of problems from acute pseudocysts. Cysts bigger than 6 cm hardly ever resolve and require internal drainage utilizing endoscopic methods. Key follow factors: persistent pancreatitis � Serum amylase and lipase levels could also be slightly elevated but marked elevations, as observed in acute pancreatitis, are unusual. Case research Case 1 A 45yearold man presents to the emergency department with a twoday history of severe periumbilical abdominal pain that was rapid in onset and has become progressively worse. He does report having had intermittent episodes of proper higher quadrant belly ache for the previous year that may often happen after meals but would at all times resolve. On bodily examination his coronary heart rate is 120, blood strain is 90/50, respiratory fee is 22, and temperature is 38.
Buy tadalis sx with a mastercard. Benefits of Garlic And Honey For Erectile Dysfunction.