|
"Order 30 gm himcolin amex, erectile dysfunction at age 23". P. Jaffar, M.B. B.CH., M.B.B.Ch., Ph.D. Co-Director, University of Arizona College of Medicine – Tucson
By definition erectile dysfunction only with partner himcolin 30 gm visa, persons with latent syphilis have serological evidence of syphilis (nontreponemal and treponemal testing) in the absence of clinical manifestations erectile dysfunction injection medication buy generic himcolin 30gm online. Early latent syphilis is defined by evidence of infection during the preceding year by 1 best erectile dysfunction pills side effects generic himcolin 30 gm overnight delivery. A documented seroconversion or four-fold or greater increase in nontreponemal titer; or 2 Symptoms of primary or secondary syphilis; or 3 erectile dysfunction 32 years old discount himcolin 30gm with visa. Laboratory testing is helpful in supporting the diagnosis of neurosyphilis; however, no single test can be used to diagnose neurosyphilis. Treatment can prevent disease progression in the individual and transmission to a partner. Persons who have had sexual contact with a person who receives a diagnosis of primary, secondary, or early latent syphilis more than 90 days before the diagnosis should be treated presumptively for early syphilis if serologic test results are not immediately available and the opportunity for follow-up is uncertain. If serologic tests are positive, treatment should be based on clinical and serologic evaluation and stage of syphilis. Sexual partners of infected persons considered at risk of infection should be notified of their exposure and the importance of evaluation. The use of any alternative penicillin treatment regimen should be undertaken only with close clinical and serologic monitoring. Limited clinical studies and biologic and pharmacologic evidence suggest that ceftriaxone may be effective; however, the optimal dose and duration of therapy have not been determined. Although systemic steroids are used frequently as adjunctive therapy for otologic syphilis, such therapy has not been proven beneficial. Because neurosyphilis treatment regimens are of shorter duration than those used in late-latent syphilis, 2. Syphilis treatment recommendations are also available in the 2015 Centers for Disease Control and Prevention Sexually Transmitted Disease Treatment Guidelines. If clinical signs or symptoms recur or there is a sustained four-fold increase in non-treponemal titers of greater than 2 weeks, treatment failure or re-infection should be considered and managed per recommendations (see Managing Treatment Failure). The potential for re-infection should be based on the sexual history and risk assessment. Response to therapy for late latent syphilis should be monitored using non-treponemal serologic tests at 6, 12, 18, and 24 months to ensure at least a four-fold decline in titer, if initially high (1:32), within 12 to 24 months of therapy. However, data to define the precise time intervals for adequate serologic responses are limited. Most persons with low titers and late latent syphilis remain serofast after treatment often without a four-fold decline in the initial titer. If clinical symptoms develop or a four-fold increase in nontreponemal titers is sustained, then treatment failure or re-infection should be considered and managed per recommendations (see Managing Treatment Failure). The potential for reinfection should be based on the sexual history and risk assessment. Antipyretics can be used to manage symptoms but have not been proven to prevent this reaction. The Jarisch-Herxheimer reaction occurs most frequently in persons with early syphilis, high non-treponemal antibody titers, and prior penicillin treatment. Managing Possible Treatment Failure or Re-infection Re-treatment should be considered for persons with early-stage syphilis who have persistent or recurring clinical signs or symptoms of disease, or a sustained four-fold increase in serum non-treponemal titers after an initial four-fold decrease following treatment. The assessment for potential reinfection should be informed by a sexual history and syphilis risk assessment including information about a recent sexual partner with signs or symptoms or recent treatment for syphilis. However, assessing serologic response to treatment can be difficult, as definitive criteria for cure or failure have not been well established. Persons whose non-treponemal titers do not decrease four-fold with 12 to 24 months of therapy can also be managed as a possible treatment failure. Targeted mass treatment of high-risk populations with azithromycin has not been demonstrated to be effective. Pregnant women with reactive treponemal screening tests should have additional quantitative testing with non-treponemal tests because titers are essential for monitoring treatment response. If the non-treponemal test is negative and the prozone reaction is ruled out, then the results are discordant; a second treponemal test should be performed, preferably on the same specimen (see Diagnosis section above). Rates of transmission to the fetus and adverse pregnancy outcomes for untreated syphilis are highest with primary, secondary, and early-latent syphilis and decrease with increasing duration of infection. Pregnancy does not appear to alter the clinical course, manifestations, or diagnostic test results for syphilis infection in adults.
Diseases - Richieri Costa Gorlin syndrome
- Prosopamnesia
- Muscular dystrophy limb-girdle with beta-sarcoglycan deficiency
- Epidermodysplasia verruciformis
- Normokalemic periodic paralysis
- Optic atrophy opthalmoplegia ptosis deafness myopia
- Sulfite oxidase deficiency
- Brachydactyly scoliosis carpal fusion
- Larsen syndrome, recessive type
- Subcortical laminar heterotopia
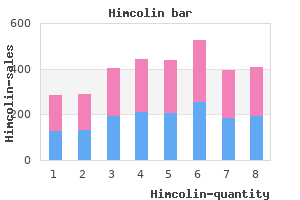
It is recognized that often the coexistence of several factors is required for the occurrence of a disease erectile dysfunction medication otc buy himcolin 30gm otc. The word cause is the one in general usage in connection with matters considered in this study erectile dysfunction topical treatment order 30 gm himcolin free shipping. It should be said at once erectile dysfunction causes cycling cheap 30gm himcolin with visa, however impotence urologist purchase 30gm himcolin overnight delivery, that no member of this Committee used the word "cause" in an absolute sense in the area of this study. Although various disciplines and fields of scientific knowledge were represented among the membership, all members shared a common conception No member was so naive of the multiple etiology of biological processes. All were thoroughly aware of the fact that there are series of events in occurrences and developments in these fields. Non-Neoplastic Res iratory Diseases, Particularly Chronic Bronchitis and Pu Pmonary Emphysema. Expected and observed deaths for smokers of cigarettes only and mortality ratios in seven prospective studies. The potential hazard is great because these diseases are major In 1962, over 500,000 people in the United of death and disability. The numbers of deaths in some important disease categories that have been reported to have a relationship with tobacco use are shown in Table 1. This table presents one aspect of the size of the potential hazard; the degree of association with the use of tobacco will be discussed later. Another cause for concern is that deaths from some of these diseases have been increasing Lung cancer In the short with great rapidity over the past few decades. While part of the rising trend for lung cancer is attributable to improvements in diagnosis and the changing age-composition and size of the population, the evidence leaves little doubt that a true increase in lung cancer has taken place. Deaths from arteriosclerotic, coronary, and degenerative heart disease rose from 273,000 in 194. Reported deaths from chronic bronchitis and emphysema rose from 2,300 in 1945 to 15,000 in 1962. The changing patterns and extent of tobacco use are a pertinent aspect of the tobacco-health problem. Cigarette consumption in the United States has increased markedly since turn of the Century, when per capita consumption was less than 50 cigarettes a year. Since 1910, when cigarette consumption per person (15 years older) was 138, it rose to 1,365 in 1930, to 1,828 in 1940, to 3,322 in 1950, and to a peak of 3,986 in l%l. The 1955 Current Population Survey showed that 68 percent of the male population and 32. In contrast with this sharp increase in cigarette smoking, per capita of tobacco in other forms has gone down. Use of chewing tobacco has declined from about four pounds per person in 1900 to half a pound in 1962. It was in this setting that the Committee began its work to assess the nature and magnitude of the health hazard attributable smoking. Seven of these compounds (polycyclic aromatic compounds) have established as cancer-producing (carginogenic), Other substances in tobacco and smoke, though not carcinogenic themselves, promote cancer production or lower the threshold to a known carcinogen. Several toxic or irritant gases contained in tobacco smoke produce experimentally the kinds of non-cancerous damage seen in the tissues and cells of heavy smokers. This includes 26 suppression of ciliary action that normally cleanses the trachea and bronchi, damage to the lung air sacs, and to mucous glands and goblet cells which produce mucus. Three kinds of cellular changes-loss of ciliated cells, thickening (more than two layers of basal cells), and presence of atypical cells-are much more common in the lining layer (epithelium) Some of the trachea and bronchi of cigarette smokers than of non-smokers. Cellular changes regularly found at autopsy in patients with chronic bronchitis are more often present in the bronchi of smokers than non-smokers. Pathological changes in the air sacs and other functional tissue of the lung (parenchyma) have a remarkably close association with past history of cigarette smoking. In retrospective studies, the smoking histories of persons with a specified disease (for example, lung cancer) are compared with those of appropriate control groups without the disease. For lung cancer alone, 29 such retrospec tive studies have been made in recent years. Despite many variations in design and method, all but one (which dealt with females) showed that proportionately more cigarette smokers are found among the lung cancer patients than in the control populations without lung cancer.
Efficacy and safety of exchange transfusion as an adjunct therapy for severe Plasmodium falciparum malaria in nonimmune travelers: a 10-year singlecenter experience with a standardized treatment protocol causes of erectile dysfunction include buy 30 gm himcolin. Typical symptoms at presentation include erectile dysfunction 60 purchase 30 gm himcolin free shipping, but are not limited to wellbutrin erectile dysfunction treatment discount himcolin 30 gm mastercard, monocular visual loss due to optic neuritis erectile dysfunction age 32 buy generic himcolin 30gm line, limb weakness or sensory loss due to transverse myelitis, double vision due to brain-stem dysfunction, or ataxia due to a cerebellar lesion. Acute demyelinating optic neuritis is the presenting feature in 15-20% of patients, and it occurs in 50% at some time. After 10-20 years, a (secondary) progressive course develops in many patients, leading to neurologic disability, but 15% of all have a progressive course from the onset of the disease. A more severe clinical course can be predicted by frequent relapses in the first 2 years, primary progressive form, male sex, and early permanent symptoms. Current management/treatment An increasing number of disease-modifying medications have become available in recent years. It is beyond the scope of this fact sheet to discuss the relative benefits, risks, modes of action, and routes of administration of these medications, except to say that all shall reduce the likelihood of the development of new white-matter lesions, clinical relapses, and stepwise accumulation of disability. Azathioprine, cyclophosphamide, or intravenous immunoglobulins are no longer part of first line treatment. If patients are unresponsive, which occurs in 20-25%, after an interval of 10-14 days a second steroid pulse in combination with therapeutic apheresis is recommended. This was shown in patients with steroid-unresponsive relapse and availability of biopsies (Stork, 2018). However, clinical, radiographic, or biomarkers that reliably differentiate immunopathological patterns or disease mechanisms are not available. Clinical improvement may not be accompanied by resolution of active lesions on imaging. Recovery of visual acuity in cases with optic neuritis was a prominent clinical result (Dorst, 2016; Koziolek, 2012). Early initiation of therapy, within 14-20 days of onset of symptoms, is a predictor of response. However, response still occurred in patients treated 60 days after the onset of symptoms. The Canadian cooperative trial of cyclophosphamide and plasma exchange in progressive multiple sclerosis. Evidence-based guideline update: plasmapheresis in neurologic disorders: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Immunoadsorption with regenerating columns in treatment of steroid refractory relapse in multiple sclerosis and optic neuritis. Response to therapeutic plasma exchange as a rescue treatment in clinically isolated syndromes and acute worsening of multiple sclerosis: a retrospective analysis of 90 patients. Immunoadsorption in steroid-refractory multiple sclerosis: clinical experience in 60 patients. Tryptophan immunoadsorption during pregnancy and breastfeeding in patients with acute relapse of multiple sclerosis and neuromyelitis optica. Relation between humoral pathological changes in multiple sclerosis and response to therapeutic plasma exchange. Therapeutic apheresis in multiple sclerosis and other central nervous system disorders. Immunoadsorption therapy in patients with multiple sclerosis with steroid-refractory optical neuritis. Heterogeneity of multiple sclerosis lesions: implications for the pathogenesis of demylination. Basic and escalating immunomodulatory treatments in multiple sclerosis: current therapeutic recommendations. Comprehensive systematic review summary: disease-modifying therapies for adults with multiple sclerosis. Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Escalation therapy of steroid refractory multiple sclerosis relapse with tryptophan immunoadsorption - observational multicenter study with 147 patients. Differences in the response to apheresis therapy of patients with 3 histopathologically classified immunopathological patterns of multiple sclerosis.
The clues to the solution of this dilemma may be first erectile dysfunction 40s purchase 30gm himcolin with mastercard, that inhalation seems to be the more important factor in the relationship between smoking and bladder cancer impotence law chennai generic himcolin 30gm on line, and secondly erectile dysfunction obesity discount himcolin 30 gm fast delivery, that other etiologic factors may have a "swamping" effect in the female to counteract her lower frequency of inhaling erectile dysfunction after radical prostatectomy treatment options 30 gm himcolin visa. The strength and specificity of the association are obviously of low order because the mean mortality ratio is 1. This also implies that factors other than smoking may be associated etiologically with urinary bladder cancer. Little can be said regarding the coherence of the association beyond the scanty data on dose-effect. Furthermore, adequate information is lacking for an intelligent discussion of the sex differential, which is the lowest for any of the cancer sites for which an association. Since there seem to be differences in patterns of smoking between rural and urban groups, additional factors must be sought to account for the lack of such a ` differential in the disease. DiPaolo and Moore utilizing different methods of preparation of the tobacco tar and different strains of mice obtained essentially negative results (75). Further retrospective studies of female cases, studies with large enough numbers of male cases to provide for further cross-classification by amount and duration of smoking and inhalation practices, and the ultimately forthcoming results on female subjects in the current Hammond prospective study will be necessary to provide more nearly adequate data in urinary bladder cancer. Conclusion Available data suggest an association between cigarette smoking and urinary bladder cancer in the male but are not sufficient to support a judgment on the causal significance of this association. The methodologv and findings of these studies have been summarized in Tables 16 and 17. Patients without gastric Not speciffrd Questioned by trained fntervlewen A,dmfssions to Raswell Park Memorid Inst. Each control group matched to mncer group by age and populstion size of place of residence. The other two studies, to date, suggested an association but these were not statistically significant (193, 325). Two of the studies did not approach the smoking variable specifically but as part of attempts to examine several possible etiological factors (94, 193); the other two were specifically directed to the role of smoking i315, 325). The mean gastric cancer mortality ratio for the seven studies is calculated to be 1. The individual studies, however, with fairly adequate numbers for stability, show a range of mortality ratios from 0. Two of the earlier reports (84,88) provide information on mortality rates or mortality ratios for the several cigarette smoking classes by amount smoked. For cigar and pipe smokers the combined studies provide a mean gastric cancer mortality ratio of 1. Carcinogenesis Squamous cell carcinoma has been produced in the forestomach of mice by the oral administration of various polycyclic aromatic hydrocarbons (8, 19, 59, 113a, 223, 276, 308, 334, 364, 368) including benzo (a) pyrene (19, 59, 276, 364). It should be noted that the forestomach of mice and rats is covered with squamous epithelium extending down from the esophagus. Stewart and Lorenz (333) produced the same type of cancer in the forestomach by injecting 20-methylcholanthrene intramurally. Rats also develop squamous cell tumors in the forestomach after prolonged oral administration of carcinogens (249). Adenocarcinoma has been produced in the glandular stomach of mice and rats by the intramural injection of carcinogenic hydrocarbons (17, 19, 187, 339) or by inserting a silk thread impregnated with 2-methylcholanthrene into the glandular stomach wall between the serosa and mucosa (332, 333). Attempts at production of cancer of the stomach with tobacco tars or condensates have not been successful (294). Eualuation of the Evidence Squamous and adeno-carcinomas have been produced experimentally in mice with benzo (a) pyrene and dibenz (a,h) anthracene injected directly into the fore- or glandular stomach. None of the retrospective studies shows an association between gastric cancer and smoking. Nor do the prospective studies yield gastric cancer mortality ratios significantly higher than the total 228 mortality ratio. In fact, the mean gastric cancer mortality ratio for cigarette smokers is below the mean total mortality ratio, and for cigar and pipe smokers it is approximately the same.
|
|